08. Idealized Continuum

The Brain Health Continuum is organized from the perspective of the individual living with a mental health condition. This continuum illuminates the phases of the experience to consider in designing the Brain Health System.
In this section of our report, we describe an idealized mental health care continuum or “blueprint.” This blueprint attempts to create a vision of what brain health care could look like as it evolves within the public sector. Many of the components of the blueprint are already in place, being delivered effectively by the Local Mental Health Authorities; however, services are unevenly distributed, have limited access and there is often a lack of smooth transitions across different parts of the mental health system (see, e.g., “Current ASH: Outpatient Service Utilization”). This blueprint was completed with consultation from the University of Texas at Austin Design Institute for Health and by working closely with our steering committees and stakeholders. The blueprint creates a substrate for developing a comprehensive vision for the care and support of people working toward recovery from mental illness.
…to design the most effective inpatient facility on the ASH Campus, a systems approach considers the hospital within the context of a complete brain health continuum…
Systems Design Approach
A system is composed of interconnected units of functionally related components. Systems design considers the whole instead of individual components in isolation. In order to design the most effective inpatient facility on the ASH Campus, a systems approach considers the hospital within the context of a complete brain health continuum, especially taking into consideration the people delivering and receiving the array of services being provided before and after an admission. This approach guides the evolution of the brain health system by creating a vision of an idealized experience for people receiving care.
Systems require all parts to be organized in a cohesive manner. A collection of services is not a system, until they are effectively integrated. Our vision for an ASH Brain Health System is organized from the perspective of the individual living with a mental health condition with the goal of helping each Texan reach optimal brain health and live his or her best life. This continuum illuminates opportunities for continuity between services at different phases of an individual’s course toward recovery.
The ASH Brain Health System Redesign focuses on the needs of youth and adults with mental health conditions who may also be living with a co-occurring intellectual disability, substance use disorder or other medical illnesses. The System must also meet the needs of family members and caregivers who play an integral role in the lives of people living with mental health challenges. The individuals the System intends to serve may be living in the community, in jail, in foster care, or on parole or probation, so these various venues were considered in the design. Because one in five people experience a mental illness, and approximately half seek care, we estimate that nearly 600,000 people are living with mental health conditions and actively needing care in the ASH Service Area (see “Epidemiologic Considerations” section). Finally, the ideal System optimizes financing to provide the best outcomes at the best cost. Expanding the scope and access of the care continuum into an integrated Brain Health System fosters earlier intervention and less reliance on expensive crisis management programs and structures.
Qualitative findings also identified a need for more effective integration with and access to care both before, during and after hospitalization, to maintain recovery following a mental health crisis.
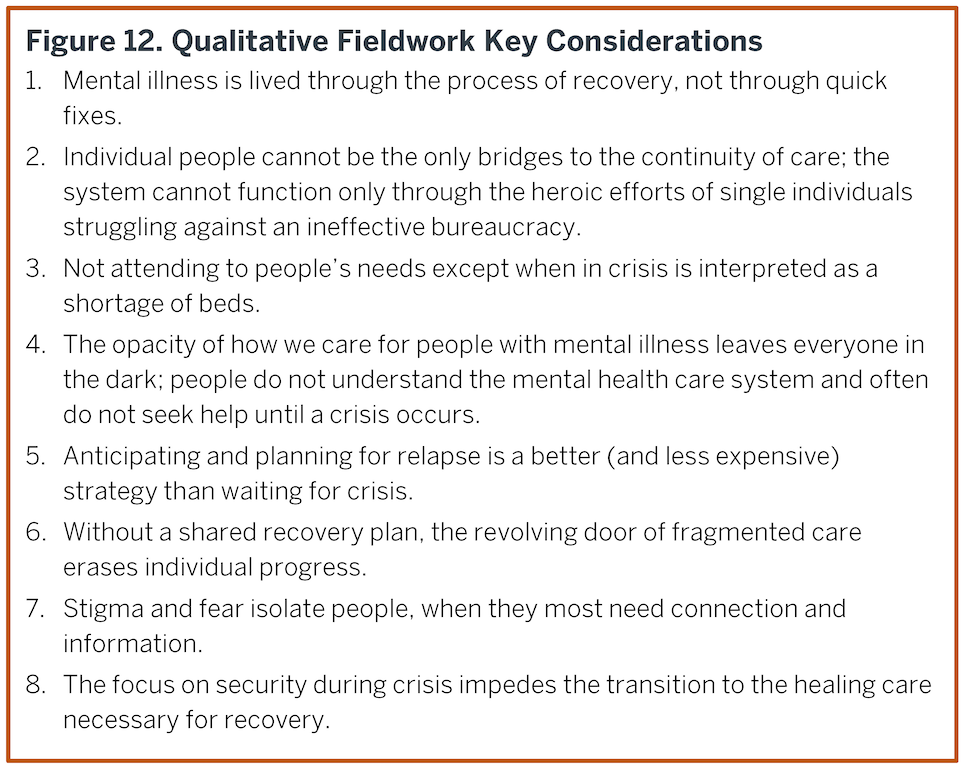
The idealized System and blueprint are largely informed by the Design Institute for Health’s qualitative fieldwork and information gathering that are provided in Appendix 10. The qualitative study gathered data from primary sources which included persons living with mental health conditions, providers, caregivers and family members, sheriffs, judges, peers, and mental health service administrators within the Austin State Hospital Service Area. Qualitative data were collected from in-person interviews, phone calls, round-table discussions, and on-site observations. The fieldwork synthesized findings into eight primary considerations, noting that consideration 1 is foundational to all the others (Figure 12); these have been edited from the original consultation to be clearer within the current context.
The qualitative findings reinforce the opportunity, first identified by the Texas Statewide Behavioral Health Strategic Plan (BHSP) (BHSPupdate), to reorganize current mental health services into a true continuum of care and recovery. Specifically, the qualitative findings suggest a need for a shared interface between a person living with mental illness and their providers across the entire care continuum. Doing so empowers an individual to optimally participate in their care, thereby driving greater connectivity, coordination, and alignment among various services. Qualitative findings also identified a need for more effective integration with and access to care both before, during and after hospitalization, to maintain recovery following a mental health crisis. Fieldwork during the study identified perceptions about the service array and system that were at odds with what the system actually delivers (e.g., the belief that there was no capacity at ASH for more youth admissions, which is not correct). Opportunities for better communication and integration will help build a continuum of care that more efficiently and effectively meets the needs of people today and reduces the overall cost of caring for people with mental illness as the population of Texas continues to grow.
ASH Brain Health System Blueprint
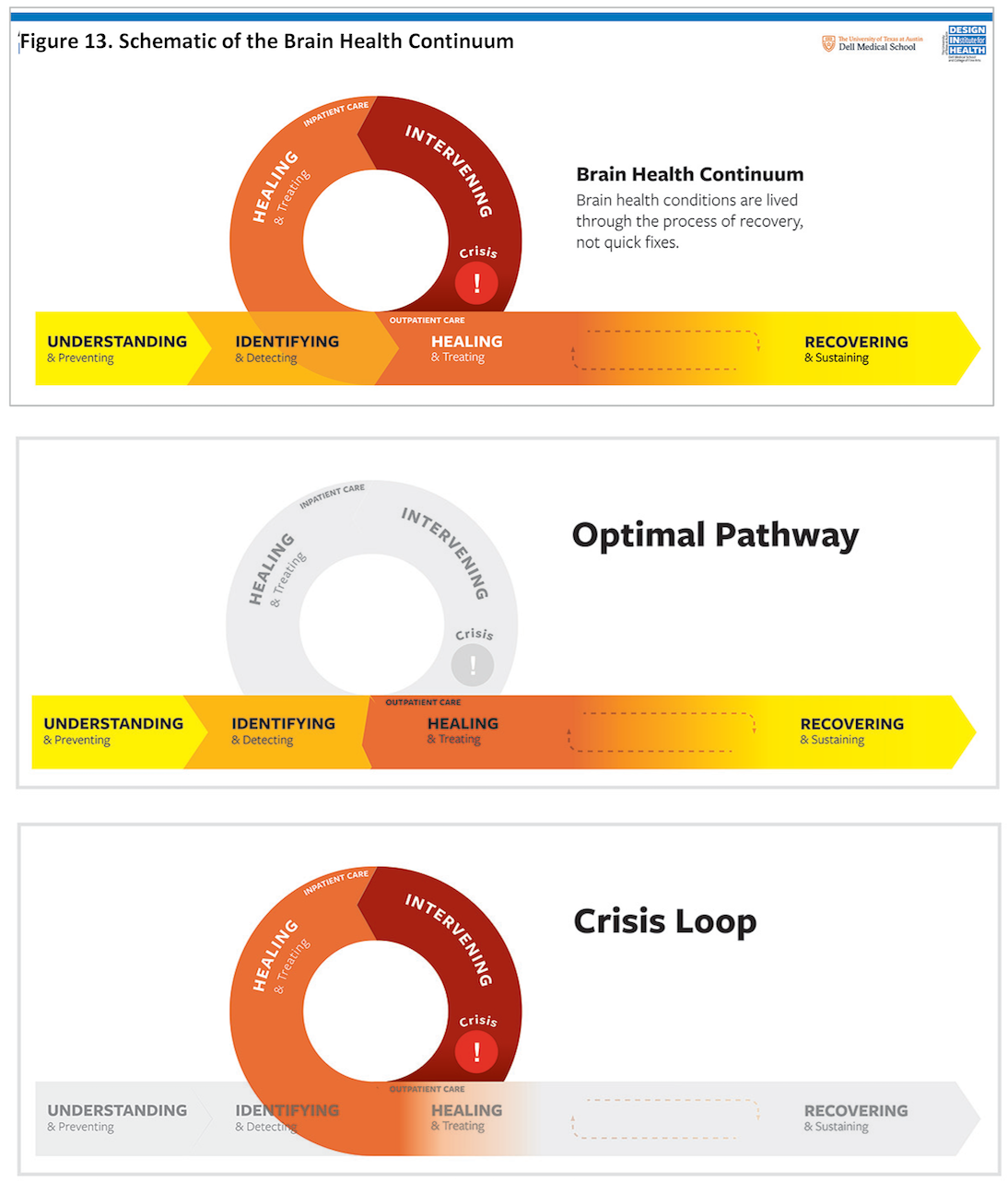
The Brain Health System Blueprint (Appendix 16) offers visual organizing principles of the key moments that shape how people experience brain health, defined by the needs of the individual rather than the services currently available (i.e. a person-centered, rather than provider-centered approach; Figure 13). This person-centered view of the system provides a foundation to expand integrated service delivery that addresses the six phases of needs expressed in the continuum. Based on the work of the Communication Strategy Subcommittee and their recommendations (Appendix 17), the names of the phases were developed collaboratively with our Peer and Family Work Group to be empowering, inclusive, and stigma free, to describe a collaborative relationship between people living with brain health conditions and the array of services.
The Blueprint offers key moments that shape how people experience brain health, defined by the needs of the individual rather than the services currently available.
The horizontal portion of the continuum represents an idealized care approach for a person living with a brain health condition. The four horizontal phases occur in the community, i.e. “outpatient” setting, where costs of clinical care are lower, brain health is relatively stable, and the overall human experience is better. The loop taking a person off the ideal pathway occurs during a mental health crisis, which generally requires emergency intervention and inpatient hospital care; it may also include law enforcement, jails, and the judicial system. The crisis loop takes a person away from their daily routine to address the crisis, but ideally with the goal of the individual returning home with a plan of how to sustain their recovery in their community.
Based upon this pathway, we developed an idealized Brain Health Continuum Blueprint to illustrate a framework of services across six phases. The services are categorized as:
1) Communication, Education, Outreach and Care;
2) Digital Tools & Innovations; and
3) Evaluation & Metrics:
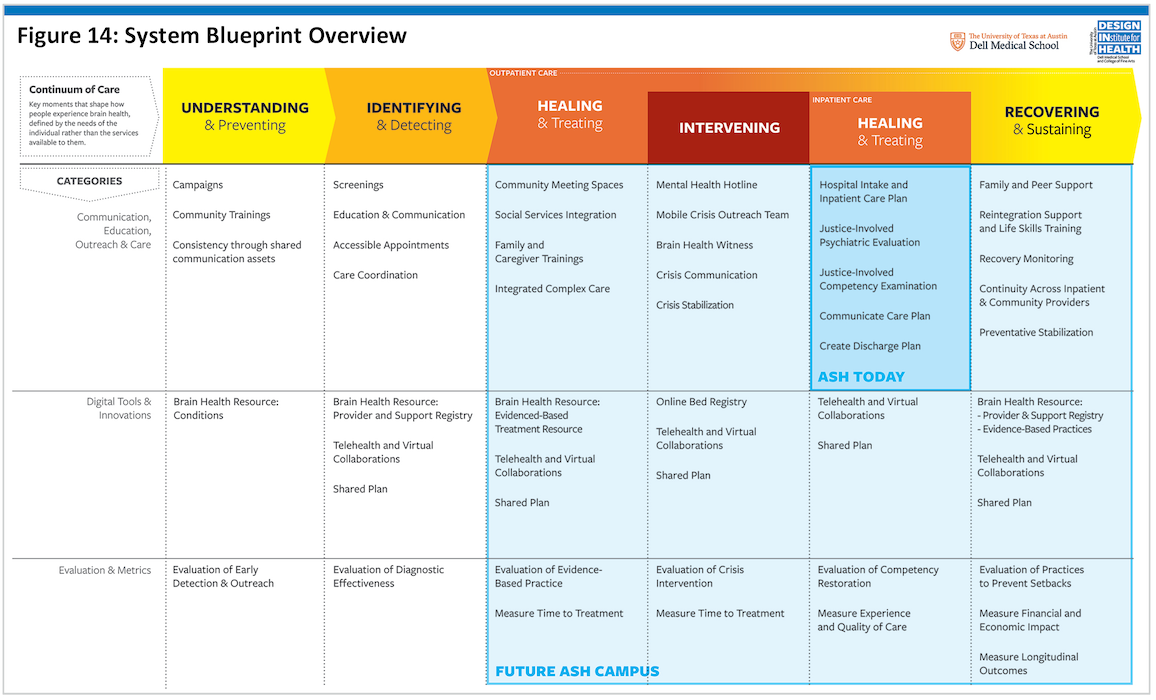
A schematic view of the System Blueprint Overview is provided in Figure 14, with an easier to read, detailed version in Appendix 16. The Blueprint identifies the portion of the care continuum that ASH delivers today, as well as the expanded set of services that a future ASH campus, including the new hospital, may deliver to provide a platform for advancing expanded care continuum across the entire Service Area. The detailed view of the System Blueprint in Appendix 16 provides descriptions of the service intents. Of note, specific providers for these services are not prescribed based on existing roles, to open the possibility of new ways of thinking about provider roles and partnerships, especially among private, public, community, and academic entities. In this regard, the Blueprint serves as a galvanizing vision for a future system that the collaborative entities across the ASH Service Area can realize together. Although details are provided in Appendix 16, we provide a brief overview of the Blueprint here, based on the organizing categories (the horizontal list across the top of the blueprint).
…the Blueprint serves as a galvanizing vision for a future system that the collaborative entities across the ASH Service Area can realize together.
Optimal Pathway
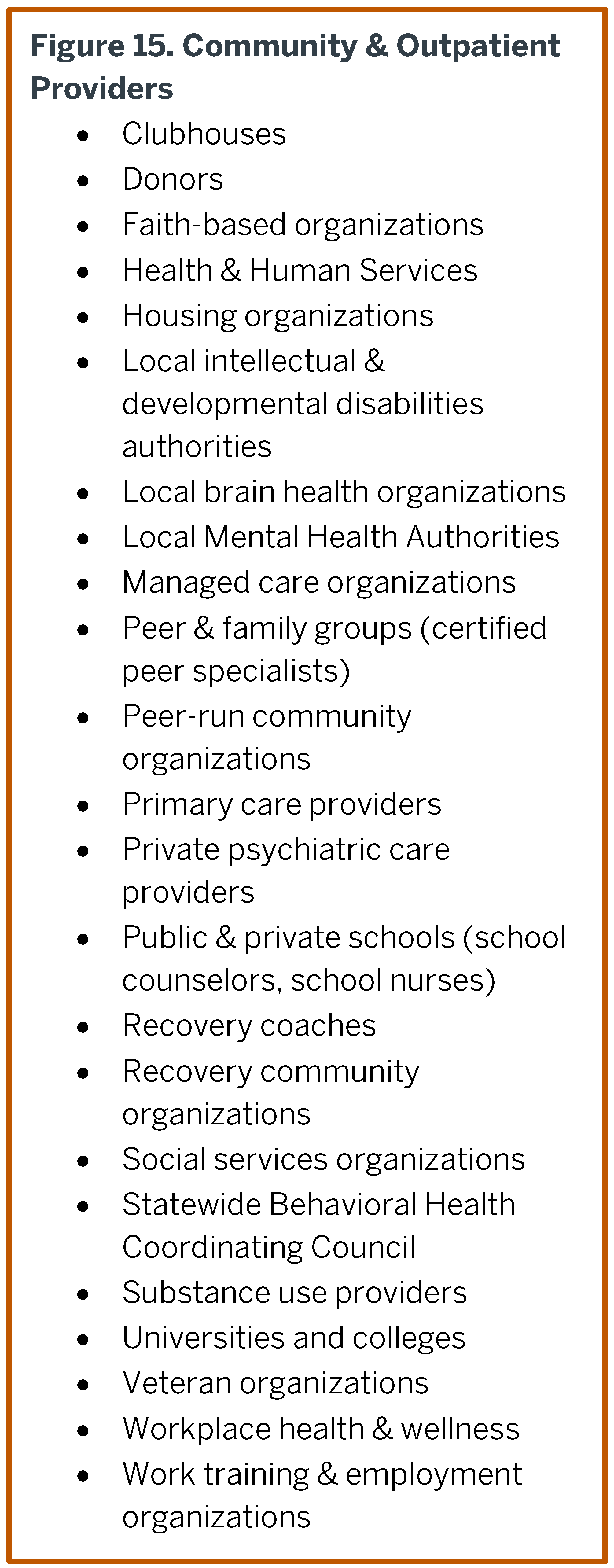
Services provided along all four phases of the optimal continuum are delivered from a wide range of community and outpatient providers (Figure 15). These entities are resources embedded in the daily lives of people across the ASH Service Area in order to integrate brain health understanding and prevention into their messages, services, and experiences.
UNDERSTANDING & Preventing
The optimal pathway begins with the need for people to be aware of brain health and mental illnesses, including prevention, risk factors, and where to find answers, care and support. Understanding and preventing applies to everyone living in the ASH Service Area, regardless of whether they have a mental health condition. Examples of services currently delivered across the ASH Service Area include Mental Health First Aid, NAMI Training, Person-Centered Recovery Training, and Outreach by Local Mental Health Authorities. The blueprint includes and expands these types of communication, education, and outreach examples with campaigns, community trainings, and shared communication assets that focus on brain health and wellness education and campaigns that reduce stigma. State investments in these programs tend to be in the form of grants focused around specific topics (e.g., Mental Health First Aid to schools).
The blueprint recommends augmenting services in Understanding & Preventing by introducing a digital “Brain Health Resource” which could provide the community with access to current information on brain health, brain health care, and illnesses/conditions in a safe and secure manner. In subsequent phases of building out the ASH Campus (beyond the current biennium), this same digital tool is used to enable information, resources, and exchanges relevant to managing brain health and preventing illness.
The blueprint envisions a series of evaluation and metrics across each phase of the continuum. Understanding & Preventing areas to assess include early detection and outreach to approaches to reduce stigma around brain health conditions and to raise knowledge for how to identify and recognize people in need early in the course of illness (before crisis). The evaluation work then convenes and coordinates cross-institution studies to advance how to communicate brain health topics and awareness to a broad audience.
IDENTIFYING & Detecting
The optimal continuum continues with a person’s need to address the early signs of a brain health condition with the help of an informed and trusted provider, including diagnosis and connections to care. Examples of services currently delivered across the ASH Service Area include screenings and diagnostic evaluations by LMHA’s, private clinicians and emergency rooms. In addition, the blueprint integrates screenings into primary care across the community and in schools (secondary through higher education).
The blueprint envisions robust and consistent communication and education with each person about his or her brain health condition(s) along with care options and/or follow up testing, regardless of ability to pay. Within public outpatient care, accessible appointments that are convenient for a person, family member, caregiver, primary care provider or school to schedule advances the continuum of care. Through care coordination, shared information, and referrals, LMHAs help people navigate to recommended care and providers. A digital brain health resource offers a provider and support resources registry across the ASH Service Area that includes feedback, ratings, and outcomes-based scores. A trusted, expert entity conducts regular inventory and assessments of providers to maintain registry.
Evaluation and metrics in this phase focus on effectiveness of screening programs and of diagnostic tools. Improvements are accomplished by convening and coordinating cross-institution longitudinal studies with people providing and receiving care on how to better detect, diagnose, and communicate a diagnosis of a mental health condition.
HEALING & Treating (Outpatient Care)
The third phase of the optimal continuum articulates how trusted, trauma-informed providers and services support a care plan that improves and sustains an individual’s health. Examples of services currently delivered include outpatient competency restoration programs, LMHA services, peer-run activities, substance use disorder programs, and adult and adolescent respite services. The blueprint enables scaling this work through community meeting spaces and social services integration.
The blueprint emphasizes the need for more in-depth family and caregiver trainings to occur in parallel and in coordination with the care a person is receiving; caregivers are key components of the healing environment, especially for youth. The blueprint emphasizes the opportunity for community providers, such as Federally Qualified Health Centers (FQHC), to integrate brain health care into primary care and complex care. A digital health resource is imagined that offers condition-specific evidence-based brain health rehabilitative and treatment practices (nationally and in the ASH Service Area). The resource is written in
accessible language and is searchable by a person’s level of motivation and engagement, location, preferences for in-person or video visits, insurance, and other factors. A number of these types of programs are in development nationally and in Texas, but have limited access. Telehealth and virtual collaborations begin at this phase and continue through the rest of the continuum, including the crisis loop. This technology equips the ASH Service Area providers with a secure forum to connect with a virtual panel of experts from an ASH telehealth center, and provide video visits to jails, schools, and emergency departments. Continued monitoring and development of technological solutions to overcome existing care shortages and barriers to access are central throughout future planning.
A shared person-centered recovery plan begins at this phase and continues through the rest of the continuum, including the crisis loop. The shared plan establishes and maintains a standard electronic interface/format for person-centered care and history that is common across providers (medical, brain health, therapists) and easy to access. This plan allows the person and caregivers to input updates, preferences, outcomes, and early indicators of relapse. The evaluation and metrics of this phase include monitoring the use of evidence-based models to connect a person with the most appropriate level of brain health care, especially during crisis.
The shared plan establishes and maintains a standard electronic interface/format for person-centered care and history that is common across providers (medical, brain health, therapists) and easy to access.
RECOVERING & Sustaining
The final phase of the optimal continuum supports individuals as they build and maintain a routine that sustains mental health wellness, builds life skills, and actively manages the signs/symptoms of a brain health condition in order to live their best possible life. Examples of services currently delivered across the ASH Service Area include clubhouse services, adult and youth day programs, supported employment, supported housing and residential living programs.
During this phase, the focus of care is on sustaining recovery and on building longitudinal relationships that can quickly intervene at the first signs of a relapse, to prevent crisis. The blueprint emphasizes peer and family support, along with life and job skills training for the person living in recovery. Some of these services are built on the ASH campus to study and advance new best models for the entire Service Area and the state.
Evaluation and metrics in this phase focus on practices to prevent recurrence and sustain brain health. This phase recognizes the need to evaluate financial and economic impact of brain health and brain health care across of the ASH Service Area. The blueprint recommends measuring longitudinal performance on outcomes for public brain health services, including LMHAs, inpatient hospitals, and collaborations with private providers and justice-involved cases.
CRISIS LOOP: INTERVENING
This phase begins when a mental health crisis creates potential for imminent danger. Providers and services involved in this phase may include:
First responders (EMT, Fire, Police)
Local sheriffs and jails
Mobile Crisis Outreach Teams (MCOT), Crisis Intervention Teams (CIT)
Emergency Room providers
Criminal & probate court judges & counselors
Probation directors
County court officials
Contracted rehabilitative brain health providers
Child protective organizations
Examples of services currently delivered for this phase includes crisis stabilization units, emergency department care, inpatient hospitalization, general hospitalization (for significant co-occurring medical illnesses), acute drug or alcohol detoxification, competency restoration and jail-based care support.
The blueprint emphasizes the need for an expanded mental health hotline that provides an easy to access, informed, single point-of-contact, multi-channel (mobile text, online chat, in person phone) 24/7 response center to consistently address emerging brain health events across Central Texas (or perhaps statewide). It coordinates the next level of care with an LMHA, the ASH, or a private psychiatric hospital. Expanded Mobile Crisis Outreach Teams are present throughout the region, supporting law enforcement to provide the best interventions in crisis. Trained peer support assists individuals entering the judicial system. Crisis communication educates each person about their brain health condition(s), and how those conditions evolve into a crisis, including any early warning signs and steps. More crises are averted by earlier intervention. An expanded network of 48 to72 hour crisis stabilization units provides additional monitored management of an illness episode and then triages individuals to the next level of care. In partnership with local courts, the system prioritizes the use of these units over legal action whenever possible. The critical digital tool for intervening is an online bed registry that establishes and maintains an ASH Service Area registry of psychiatric intensive care beds accessible to the public that is updated at least every four hours. Ideally, telehealth, virtual collaborations, and the shared recovery plan are incorporated into crisis intervention. Evaluation and metrics of crisis intervention include capacity and capability of state funded brain health crisis services across the ASH Service Area.
CRISIS LOOP: HEALING & Treating
(Inpatient Care)
This phase generally follows intervening, but may also arise from a crisis that is self-identified without intervention. This phase includes the Austin State Hospital and its core services. This phase addresses a person’s engagement with coordinated inpatient care that includes treatment services, and support. Examples of providers and services involved in this phase may include:
State hospital psychiatric care teams, administrators, staff and liaisons
Contracted private hospitals psychiatric care teams, administrators, staff
Health & Human Services Commission
State contracted rehabilitative brain health providers
Peer & Family Groups
Recovery Coaches
The blueprint envisions an inpatient recovery plan that is informed by evidence-based best practices and integrated into ongoing outpatient care. For justice-involved persons receiving care, psychiatric evaluations and competency examinations are now managed separately within the inpatient experience, as described in the “Competency Restoration” Recommendations of this report. The discharge plan coordinates an individual’s transfer to step-down care, residential options, or jail with Local Mental Health Authorities, ASH, and/or courts according to the person’s care plan, ensuring that the incoming provider team is presented the specific discharge material and recovery plan to ensure continuity of care. Discharge plans assess and source social and medical services that enhance a truly integrated holistic recovery model. Although many of these components currently exist, operational improvements are developed in the integration with hospital admission and discharge. In the blueprint, the role of expanded telehealth provides a secure forum for a person and the ASH/inpatient providers to connect with community providers, family, caregivers from an ASH telehealth center to manage a large Service Area until more local community resources are established. The shared plan provides continuity of care across community, crisis, jails, emergency rooms and inpatient facilities.
Evaluation and metrics in this phase focus on re-integration back into outpatient care. Measurement of experience and quality of care collect feedback from public, providers and persons receiving care in the ASH Service Area around overall experience, quality of care, outcomes, time to reach outcomes, and understanding of care plan.
Key Points – Idealized Brain Health System Blueprint
• Idealized mental health care system is focused on individuals receiving care while supporting those providing care and managing crises.• Various components of the continuum exist within public sector and function reasonably well under LMHAs, peace officers, and ASH, however there are still gaps with the system that can be addressed in the community.
