05. Mental Health Workforce in ASH Service Area

Photo by dusanpetkovic/iStock / Getty Images
A diverse and skilled mental health workforce is an essential element of a well-functioning public mental health system. Building larger hospitals and adding more psychiatric beds provides no value if the workforce and operational budgets supporting those beds is not similarly increased. While this capability is important for both community-based services through Local Mental Health Authorities (LMHAs) and community hospitals, it also affects the operations of the Austin State Hospital. Workforce shortages in critical positions such as psychiatrists, nurses, pharmacists, and psychiatric nursing assistants (PNA) have had a direct impact on bed availability because of licensing and accreditation standards. As noted in the “Current State: The Austin State Hospital” section of this report, ASH experiences significant turnover in these positions. In fact, ASH functioning is currently below capacity for both the number of available beds (299) and, until recently, the number of funded beds (263 in FY19), specifically because of workforce shortages.
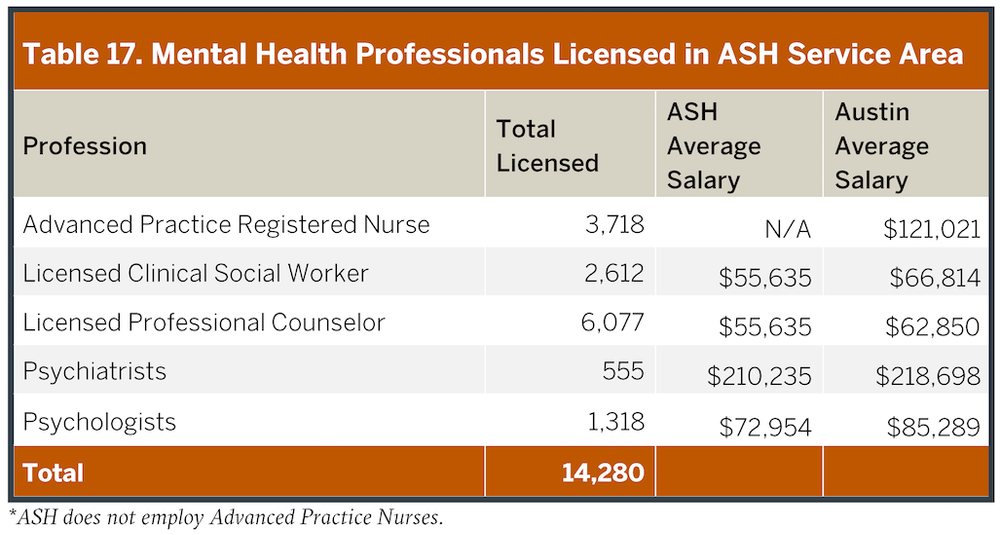
Wages for mental health employees at ASH are lower than wages for comparable positions in the community, as illustrated in Table 17. This problem is one consequence of setting wages through a large state agency rather than based on local economies. Hiring is local and if a state facility cannot offer competitive wages based upon the locale (not a statewide average), then state hospitals, like ASH, struggle to compete for the best skill employees. Indeed, low wages, coupled with aged facilities, make it difficult to attract and retain high quality new employees in critical positions.
Workforce shortages in critical positions such as psychiatrists, nurses, pharmacists, and psychiatric nursing assistants (PNA) have had a direct impact on bed availability…
In the ASH Service Area, there are less than 15,000 licensed mental health professionals, including fewer than 600 psychiatrists (Table 17). The sufficiency of a mental health workforce is typically based on the rate of providers per unit population. For example, the necessary number of psychiatrists has been defined in a recent State of Texas report as one psychiatrist for every 4,000 people; less than one psychiatrist per 30,000 people is designated as a federal Health Professional Shortage Area. In the ASH Service Area, there is one psychiatrist for every 6,700 people (based upon a population of 3.7 million). While no county in the ASH Service Area met the 4,000 person per psychiatrist standard when last computed by the state, psychiatrists are unevenly distributed across the region and tend to cluster in high-density population centers. More populated areas (like Travis County) come closer to the recommended numbers, whereas many rural counties have little or no access to a psychiatrist. Many of these professionals working in private settings, and often do not accept insurance and do not serve indigent, uninsured, or underinsured (e.g. Medicaid, Medicare) people, compounding these shortages. Similar shortages exist across the ASH Service Area for other mental health specialties.
In the ASH Service Area, there are less than 15,000 licensed mental health professionals, including fewer than 600 psychiatrists.
Multiple factors drive these shortages, but many of the counties served by ASH are rural, and rural counties struggle nationally to attract medical professionals of all types. In addition, licensing delays, particularly for psychologists moving into Texas, can significantly limit the availability of new professionals in the state. Similar delays for psychiatrists were addressed through development of expedited licensing during the last legislative session through SB(85R) 674. However, limited availability of psychiatrists remains common in most of the Service Area for LMHAs, community hospitals, and forensic settings for many of these same reasons. While telehealth has significant potential, particularly in rural areas, this technology has yet to be broadly implemented. One recent barrier to telemedicine was removed when the legislature agreed to allow telemedicine to occur without requiring a person to an initial in-person visit; for a state the size of Texas, this statutory change was critical for telemedicine and telehealth to be truly viable.
“In the ASH Service Area, there is one psychiatrist for every 6,700 people.”
In light of the competition for a scarce mental health workforce in the ASH Service Area, and the severe negative impact when bed capacity is reduced from critical staff shortages, the Texas Health and Human Services Commission (HHSC) and ASH need to explore new strategies to recruit and retain critical staff. HHSC has been increasing its efforts to establish partnerships between state hospitals and academic institutions as one approach toward this issue.
A 2016 legislative report on academic partnerships indicated that there are a number of potential workforce benefits of such collaborations, including:
Improving staff recruitment and retention,
Providing training and staff development,
Integrating services though leveraging of existing resources and relationships,
Increasing focus on best practices, and
Enhancing service delivery through innovation.
Various Texas state hospitals have arranged affiliations with academic institutions, including research and training programs, staffing agreements, and, in one case, full operational control of a public psychiatric hospital. The latter involves the Harris County Psychiatric Center (HCPC). HCPC has existed for almost four decades, and it serves over 9,000 people per year. It is operated by The University of Texas Health Science Center at Houston (UTHealth; rather than as a department in HHSC), and it receives state funding through a contract with the LMHA – The Harris Center for Mental Health and IDD (The Harris Center). HCPC provides excellent care, as indicated by its award from the Joint Commission in 2016 as a Top Performer in Key Quality Measures. HCPC had a long evolution to reach its current performance, and it is also in the process of planning for new construction as part of the HHSC Comprehensive Plan for State-Funded Inpatient Mental Health Services (Appendix 2). Staffing shortages have not been a barrier to operations at HCPC. With this model, in which HHSC and the state contract with a health-system to manage a hospital, rather than owning all operations, improved effectiveness and efficiencies are possible. Additionally, this structure allows local salary adjustments to attract a strong workforce. These considerations contributed to the final “Recommendations” of this report.
Key Points – ASH Service Area: Workforce
• Workforce instability has contributed to staffing issues at ASH and other state hospitals.• There is an inadequate mental health workforce in the ASH Service Area and challenges recruiting the existing workforce into the public system.
• Academic partners may provide one approach toward strengthening the workforce, as demonstrated by successes observed with the Harris County Psychiatric Center.
